
Introduction
Methods And Materials
A prospective descriptive analysis was done in Department of Surgery of Rajarajeswari medical college, Bangalore, India. This is a tertiary care teaching hospital mainly serving rural population. The study period was for one year from January 2017 to December 2017. All the patients admitted and operated for diabetic foot
complication were included in the study and their data was entered in study performa. The following were the exclusion criteria
1] Patients who refused surgery and were discharged against medical advice
2] Patients operated in other specialty department
3] Patients operated elsewhere
4] Patients admitted for skin grafting The study was approved by our institutional ethics committee [RRMCH-IEC/157/2016-17]
Statistical Methods:
Significant figures
+ Suggestive significance (P value: 0.05<P<0.10)
* Moderately significant ( P value:0.01<P ≤ 0.05)
** Strongly significant (P value : P≤0.01)
Statistical software: The Statistical software namely SPSS 18.0, and R environment ver.3.2.2 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
Results
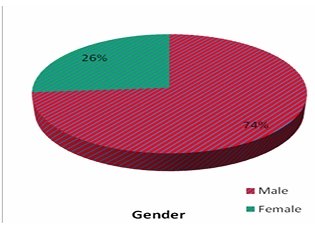
total of 61 patients were included in this study. Majorityof the patients were males [73.8%] in this study [Table 3]. Most patients were in age [Table 4] ranging from 5 to 60 years [56.92+/-11.92]. Left foot was the commonest side involved affecting 38 patients [62.3%].
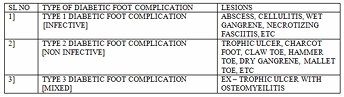
Wet gangrene [Table 5] was most common pathological lesion seen in 24.6% followed by abscess [Fifure 1]] which was seen in 23%. Majority of the patients thus
belonged to Type 1 diabetic foot complications [67.2%] followed by type 3 diabetic foot complication [29.5%] and it was statistically significant (P<0.001). Debridement is the most common surgical procedure done [Table 6]. 32 patients [52.5%] had some type of amputation being performed. There was no significant association between amputation done [Table 7] and type of diabetic foot Amit Kumar C Jain, et al. International Journal of Medical Sciences and Innovative Research (IJMSIR)
© 2018 IJMSIR, All Rights Reserved
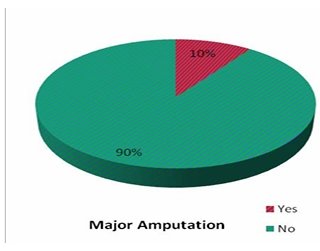
complication [P+0.241]. Among amputations, 6 patients [9.8%] had major amputation [Table 8].
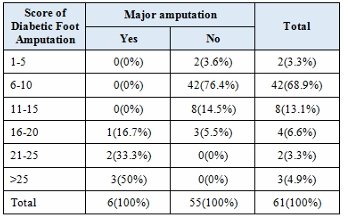
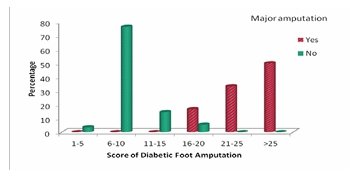
Majority of diabetic foot patients [68.9%] had a score between 6 to 10 and were in low risk category of major amputation. It was seen that, with increasing score, the risk of major amputation [Table 9] increased significantly [P<0.001]. There were 6 major amputation with all having score above 16. All patients who had score above 25 invariably had major amputation done. Patients with type 2 diabetic foot complication [Table 10] had higher scores compared to other complication suggesting significance [19.50+/-10.61, P-0.040].
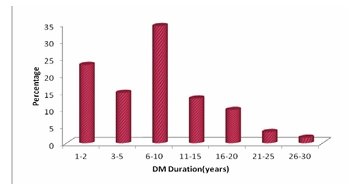
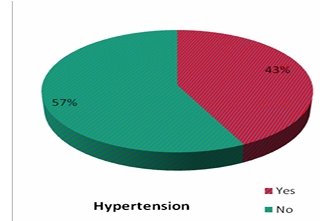
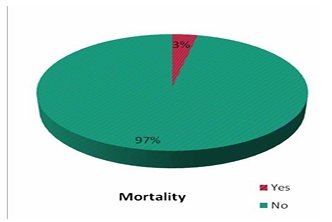
.Majority of patients [34.4%] had diabetes [Table 11] of 6-10 years duration [8.57+/- 6.68]. 42.6% had associated hypertension [Table 12], 4.9% had chronic kidney disease [Table 13] and 9.8% had ischemic heart disease [Table 14]. It was seen that patients with type 3 diabetic foot complication had longer duration of diabetes suggesting some significance [10.89+/-7.53, P-0.088]. There were two mortality [Table 15] in this study and it was associated with high scores {22.00+/-11.31, P<0.001} and it was statistically significant [Table 16].
Discussion
Various classifications and scoring system have been proposed in diabetic foot with most of them focusing only on diabetic foot ulcers [2, 5, 7, 8]. Some of the classifications are Wagner’s classification, University of Texas classification, PEDIS classification whereas some of the known scoring system are DEPA scoring system, DUSS, etc [2, 5, 7, 8, 11, 12].
It is now clear that there is a difference between a classification and a scoring system [12]. A classification is descriptive in nature, whereas a score is a numerical descriptor and is usually meant to provide an idea of severity [12]. It is also well known that it is very difficult for a single classification system to effectively serve both these purposes [12]. Therefore, the current study employed Amit Jain’s classification for diabetic foot complications along with Amit Jain’s scoring system, which predicts the risk of major amputation in diabetic foot complications [7,8,9,10].
The Amit Jain’s classification for diabetic foot complications was first proposed in 2017 and was the first classification to encompass all lesions seen universally [7,8,13,14]. Initially, no studies were conducted on this classification at the time of its proposal [7]. Subsequently, many new studies evaluated this classification, and various studies demonstrated that type 1 diabetic foot complications were the most common cause of hospital admission [13,14,15]. In the series by Jain et al., it was observed that 86.67% of admitted patients had type 1 diabetic foot complications, whereas in the series by Kalaivani et al., this figure was 91.06% [13,15]. Wet gangrene and abscess were the most common lesions reported across different studies [2,13,14,15]. Similarly, in the present series, wet gangrene followed by abscess were the two most common lesions encountered. More than 67% of the patients had type 1 diabetic foot complications, which was found to be statistically significant in this study.
The majority of studies have shown that the most common reason for major amputation is type 1 diabetic foot complication [2,13,15]. In the present study as well, major amputation was most commonly associated with type 1 diabetic foot complications. In a validation study of Amit Jain’s scoring system by Kalaivani et al. [16], it was observed that more than 85.7% of patients who underwent major amputation had a score greater than 16. Similarly, in the series by Jain et al., more than 80% of patients with major amputation had a score of 16 or above [17].
In our series, we found a significant association between Amit Jain’s scoring system and major amputation, with higher scores being associated with an increased incidence of major amputations. Furthermore, a significant association was also observed between higher scores and mortality. Type 2 diabetic foot complications demonstrated significantly higher scores overall when compared to other types of diabetic foot complications. In the series by Jain et al. [17] on the scoring system, mortality was similarly associated with higher scores. Additionally, stump complications following major amputation were more commonly observed in patients with type 1 diabetic foot complications and were predominantly seen in those with higher scores, as reported in earlier studies [10]. Despite the numerous studies conducted on Amit Jain’s classification over the past four to five years, a recent review by Nather et al. [18] on diabetic foot classifications failed to analyze or include these studies on Amit Jain’s classification.
Conclusion
References
Gulf Diabetic Foot Working Group. Identification and management of infection in diabetic foot ulcers: International Consensus. Wounds International. 2017.
Singh M, Sahu A. Analyzing diabetic foot complication according to modern comprehensive Amit Jain classification from Indian subcontinent in a government care setting. IJCMAAS. 2017;13(3):125–130.
Doupis J, Veves A. Classification, diagnosis and treatment of diabetic foot ulcers. Wounds. 2008;20(6).
Jeffcoate WJ, Chipchase SY, Ince P, Game FL. Assessing the outcome of the measurement of diabetic foot ulcers using ulcer-related and personal-related measures. Diabetes Care. 2006;29:1784–1787.
Dhubaib H. Understanding diabetic foot complications: In praise of Amit Jain’s classification. Diabetic Foot Journal Middle East. 2015;1(1):10–11.
Parisi MCR, Wittmann DEZ, Pavin EJ, et al. Comparison of three systems of classification in predicting the outcome of diabetic foot ulcers in a Brazilian population. European Journal of Endocrinology. 2008;159:417–422.
Jain AKC. A new classification of diabetic foot complications: A simple and effective teaching tool. Journal of Diabetic Foot Complications. 2012;4(1):1–5.
Jain AKC, Joshi S. Diabetic foot classifications: Review of literature. Medicine Science. 2013;2(3):715–721.
Jain AKC. The new scoring system for predicting the risk of major amputations in patients with diabetic foot complications. Medicine Science. 2014;3(1):1068–1078.
Jain AKC, Viswanath S. Analysis of stump complications following major amputation in diabetic foot complications using Amit Jain’s principle and practice for diabetic foot. Scholars Journal of Applied Medical Sciences. 2016;4(3E):986–989.
Rosner B. Fundamentals of Biostatistics. 5th ed. Duxbury; 2000:80–240.
Riffenburg RH. Statistics in Medicine. 2nd ed. Academic Press; 2005:85–125.
Sunder Rao PSS, Richard J. An Introduction to Biostatistics: A Manual for Students in Health Sciences. 4th ed. New Delhi: Prentice Hall of India; 2006:86–160.
Suresh KP, Chandrasekhar S. Sample size estimation and power analysis for clinical research studies. Journal of Human Reproductive Sciences. 2012;5(1):7–13.
Schaper NC. Diabetic foot ulcer classification systems for research purposes: A prognosis report on criteria for including patients in research studies. Diabetes/Metabolism Research and Reviews. 2004;20(Suppl 1):S90–S95.
Game F. Classification of diabetic foot ulcers. Diabetes/Metabolism Research and Reviews. 2016;32(1):186–194.
Jain AKC, Viswanath S. Distribution and analysis of diabetic foot. OA Case Reports. 2013;2(21):117.
Singh M, Singh AR. Evaluation and management of diabetic foot complications using Amit Jain’s classification: An exploration of use. Diabetic Foot Journal Middle East. 2016;2(1):16–19.
Kalaivani V. Evaluation of diabetic foot complications according to Amit Jain’s classification. Journal of Clinical and Diagnostic Research. 2014;8(12):7–9.
Kalaivani V, Melanta K. Application of Amit Jain’s scoring system in diabetic foot amputees. Journal of Evolution of Medical and Dental Sciences. 2016;5(28):1413–1417.
Jain AKC, Viswanath S. Studying major amputation in a developing country using Amit Jain’s typing and scoring system for diabetic foot complications: Time for standardization of diabetic foot practice. International Surgery Journal. 2015;2(1):26–30.
Nather A, Jun WY, Juan SL. Choosing a classification for the management of patients with diabetic foot problems. Orthopaedic Surgery and Traumatology. 2017;1(3):104–110.
FIGURES

Tables and Graphs
| SL. NO | CHARACTERISTICS | INVOLVEMENT OF FOOT | |||
|---|---|---|---|---|---|
| 1] | PRESENCE OF ULCER | NO ULCER → 0 | FOOT ULCER → 2 | MIDFOOT ULCER → 4 | HINDFOOT ULCER / FULL FOOT / BEYOND → 6 |
| 2] | OSTEOMYELITIS (O.M) | NO O.M → 0 | FOREFOOT O.M → 2 | MIDFOOT O.M → 4 | HINDFOOT O.M → 6 |
| 3] | PRESENCE OF PUS | NO PUS → 0 | FOREFOOT PUS / DORSUM → 2 | MIDFOOT PUS → 4 | HINDFOOT PUS / BEYOND IT → 6 |
| 4] | GANGRENE (DRY / WET) | NO GANGRENE → 0 | FOREFOOT GANGRENE → 2 | MIDFOOT GANGRENE → 4 | HINDFOOT GANGRENE / BEYOND → 8 |
| 5] | PERIPHERAL ARTERIAL DISEASE | NO P.A.D → 0 | MILD → 2 | MODERATE → 4 | SEVERE → 8 |
| 6] | CHARCOT FOOT / DESTROYED JOINTS | NO → 0 | FOREFOOT → 2 | MIDFOOT → 4 | HINDFOOT / WHOLE FOOT → 8 |
| 7] | NECROSIS (SKIN) | NO → 0 | FOREFOOT NECROSIS → 2 | MIDFOOT NECROSIS → 4 | HINDFOOT NECROSIS / BEYOND → 8 |
| 8] | ASSOCIATED CELLULITIS | NO → 0 | UPTO FOREFOOT → 2 | UPTO MIDFOOT → 4 | UPTO HINDFOOT & BEYOND → 6 |
| 9] | PREVIOUS AMPUTATION | NO → 0 | TOE AMPUTATION | FOREFOOT AMPUTATION | MIDFOOT AMPUTATION → 6 |
| 10] | PRESENCE OF GAS RADIOLOGICA LLY N | NO → 0 | AS IN FOREFOOT 1 | GAS IN/UPTO MIDFOOT 2 | AS IN/UPTO HINDFOOT → 3 |
| Gender | No. of patients | % |
|---|---|---|
| Male | 45 | 73.8 |
| Female | 16 | 26.2 |
| Total | 61 | 100.0 |
| Age in years | No. of patients | % |
|---|---|---|
| 30–40 | 4 | 6.6 |
| 41–50 | 19 | 31.1 |
| 51–60 | 16 | 26.2 |
| 61–70 | 15 | 24.6 |
| >70 | 7 | 11.5 |
| Total | 61 | 100.0 |
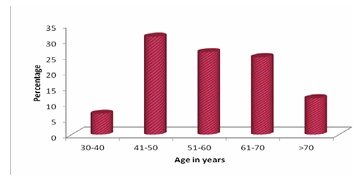
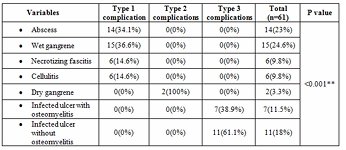
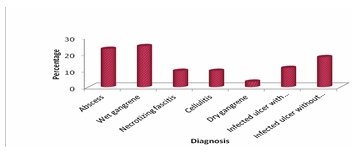
Table 6: Surgery distribution of patients studied
| Surgery | No. of patients | % |
|---|---|---|
| Debridement | 29 | 47.5 |
| Toe amputations | 15 | 24.6 |
| Transmetatarsal amputation | 11 | 18.0 |
| Below knee amputation | 2 | 3.3 |
| Above knee amputation | 4 | 6.6 |
| Total | 61 | 100.0 |
| Amputati on done | 1 | 2 | 3 | Total |
|---|---|---|---|---|
| yes | 19(46.3 %) | 2(100 %) | 11(61.1 %) | 32(52.5 %) |
| No | 22(53.7 %) | 0(0%) | 7(38.9%) | 29(47.5n %) |
| Total | 41(100%) | 2(100%) | 18(100%) | 16(100%) |
| Major Amputation | No. of patients | % |
|---|---|---|
| yes | 6 | 9.8 |
| No | 55 | 90.2 |
| Total | 61 | 1000 |
| Variables | Type of Complications 1 | Type of Complications 2 | Type of Complications 3 | Total | P value |
|---|---|---|---|---|---|
| Age (years) | 56.93 ± 12.05 | 53.00 ± 10.24 | 57.33 ± 12.51 | 56.92 ± 11.92 | 0.891 |
| DM Duration | 7.90 ± 6.11 | 1.50 ± 0.71 | 10.89 ± 7.53 | 8.57 ± 6.68 | 0.08+ |
| Score of Diabetic Foot Amputation | 10.07 ± 5.47 | 19.50 ± 10.61 | 9.11 ± 4.50 | 10.10 ± 5.55 | 0.04* |
| DM Duration (years) | No. of patients | % |
|---|---|---|
| 1–2 | 14 | 23.0 |
| 3–5 | 9 | 14.8 |
| 6–10 | 21 | 34.4 |
| 11–15 | 8 | 13.1 |
| 16–20 | 6 | 9.8 |
| 21–25 | 2 | 3.3 |
| 26–30 | 1 | 1.6 |
| Total | 61 | 100.0 |
| Hypertension | No. of patients | % |
|---|---|---|
| yes | 26 | 42.8 |
| No | 35 | 57.4 |
| Total | 61 | 1000 |
| CKD | No. of patients | % |
|---|---|---|
| yes | 3 | 4.9 |
| No | 58 | 95.1 |
| Total | 61 | 1000 |
| IHD | No. of patients | % |
|---|---|---|
| yes | 6 | 9.8 |
| No | 55 | 90.1 |
| Total | 61 | 1000 |
| Mortality | No. of patients | % |
|---|---|---|
| yes | 2 | 3.3 |
| No | 59 | 96.7 |
| Total | 61 | 1000 |
| variables | Yes | No | Total | P value |
|---|---|---|---|---|
| Score of Diabetic Foot Amputation | 22.00± 11.31 | 9.69±4.9 6 | 10.10±5.5 5 | 0.001* * |

