Conclusion : In this validation study, it is seen that majority of the Charcot foot in clinical practice were
of simple type and surgeries were done in type 3 Charcot foot. All the major amputation occurred in type
3 Charcot foot and osteomyelitis had significant association with amputation. There was no mortality in
this study. Amit Jain’s classification for Charcot foot is a simple, practical, easy to remember focal
classification that guides therapy, serves a good teaching and communicative tool.
Keywords: Diabetes, charcot, amit jain, ulcer, amputation, classification, foot
Introduction
Charcot foot, which is also known as Charcot neuropathic arthropathy, is a progressive,
inflammatory, noninfectious, destructive disease that affects foot and ankle. [1, 2, 3] This
condition can result in fractures, subluxation, dislocation, deformities and can result in limb
loss [1, 3, 4, 5].
This condition was first described by Jean Martin Charcot in 1868 in case of tabes dorsalis and in the year 1936, William Riley Jordan noticed its association with diabetes [2, 5, 6]. There are various different classifications for Charcot foot based on radiological features, Clinical, anatomical involvement, etc. [2, 6, 7, 8] Some of the well-known Charcot foot classifications are Eichenholtz, Dounis, Roger’s- Bevilacqua, Sander’s- Frykberg’s, Sella- Barrette classification, etc [2, 6, 7, 8, 9]. All of these novel classifications have their own different merits and are used in different parts of the world.
Amit Jain’s classification for Charcot foot is a newly proposed classification for Charcot foot(Table 1) which is an extension of “SCC” classification concept that was first proposed for diabetic foot ulcer in 2014 [8, 10, 11]. This concept of “Simple, Complex, Complicated” classification system was later extended to Amit Jain’s classification for diabetic foot classifications, offloading, callosity, therapeutic foot wear, toe deformities, foot amputations and Charcot foot [8, 12, 13, 14].
The e “SCC” classification concept is a component of Amit Jain’s system of practice which is a modern diabetic foot surgery concept that was developed by the primary author [8, 15]. The objective of this present study was to analyze the Amit Jain’s extended “SCC” classification for Charcot foot [Figure 1] and describe the results and outcomes associated with this new classification.
This condition was first described by Jean Martin Charcot in 1868 in case of tabes dorsalis and in the year 1936, William Riley Jordan noticed its association with diabetes [2, 5, 6]. There are various different classifications for Charcot foot based on radiological features, Clinical, anatomical involvement, etc. [2, 6, 7, 8] Some of the well-known Charcot foot classifications are Eichenholtz, Dounis, Roger’s- Bevilacqua, Sander’s- Frykberg’s, Sella- Barrette classification, etc [2, 6, 7, 8, 9]. All of these novel classifications have their own different merits and are used in different parts of the world.
Amit Jain’s classification for Charcot foot is a newly proposed classification for Charcot foot(Table 1) which is an extension of “SCC” classification concept that was first proposed for diabetic foot ulcer in 2014 [8, 10, 11]. This concept of “Simple, Complex, Complicated” classification system was later extended to Amit Jain’s classification for diabetic foot classifications, offloading, callosity, therapeutic foot wear, toe deformities, foot amputations and Charcot foot [8, 12, 13, 14].
The e “SCC” classification concept is a component of Amit Jain’s system of practice which is a modern diabetic foot surgery concept that was developed by the primary author [8, 15]. The objective of this present study was to analyze the Amit Jain’s extended “SCC” classification for Charcot foot [Figure 1] and describe the results and outcomes associated with this new classification.
Table 1 Showing the Amit Jain’s e”SCC classification for Charcot foot
| Type of Charcot foot | Description | Clinical characteristics | Treatment guidelines |
|---|---|---|---|
| Type 1 Charcot foot | Simple Charcot foot | Charcot foot without ulcer (acute/chronic) | TCC/RCW Acute Charcot foot , Modified footwear Chronic Charcot foot |
| Type 2 Charcot foot | Complex Charcot foot | Charcot foot with ulcer | Offloading, Standard wound care, Surgery like Exostectomy if recurrent ulcer |
| Type 3 Charcot foot | Complicated Charcot foot | Charcot foot with infection or instability | Surgery like debridement, removal of infected bone, antibiotics, Reconstructive surgery for unstable Charcot foot, Offloading, Standard wound care |
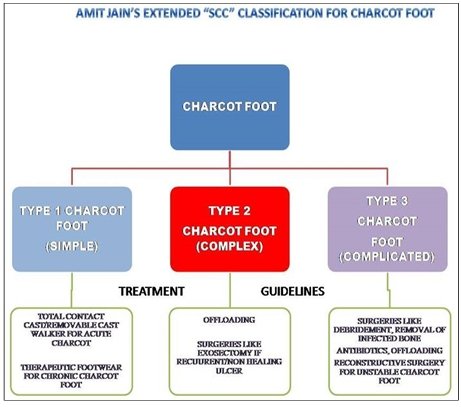
Fig 1: Showing the Amit Jain’s classification for Charcot foot
Materials and Methods
A descriptive retrospective analysis was carried out at 2 center’s
namely Amit Jain’s Institute of Diabetic Foot and Wound Care,
Brindhavvan Areion hospital and at Department of Surgery of
Rajarajeswari medical college, Bengaluru, India. The study
period was from May 2017 to April 2019. The charts and
records were reviewed to obtain demographic profile,
radiological features and surgeries done. The following were
inclusion and exclusion criteria.
Inclusion criteria
1. All patients who were treated for Charcot foot in Diabetes
Exclusion criteria
1. Non-diabetics with Charcot foot
2. Patients admitted in other departments
3. Patients who refused treatment
4. Patients with insufficient data
IEC approval was obtained for this study from Rajarajeswari
medical college ethics committee [RRMCH-IEC/43/2018-19]
Statistical analysis [16, 17, 18, 19]
Data was analyzed using statistical software SPSS 22 and R
environment Ver. 3.2.2. Microsoft word and excel were used for
general graphs and tables. Both descriptive and inferential
statistical analysis was carried out in this study. Results on
continuous measurements are presented on Mean SD (Min-Max)
and results on categorical measurements are presented in
number (%). Significance is assessed at 5% level of significance.
The assumptions made on data are that the dependent variables
should be normally distributed, samples drawn from the
population should be random and cases of the samples should be
independent. Student t test (two tailed, independent) has been
used to find the significance of study parameters on continuous
scale between two groups (Inter group analysis) on metric
parameters. Leven`s test for homogeneity of variance has been
performed to assess the homogeneity of variance. Chi-square/
Fisher Exact test has been used to find the significance of study
parameters on categorical scale between two or more groups,
Non-parametric setting for Qualitative data analysis. Fisher
exact test was used when samples were very small.
Significant figures
1. Suggestive significance (P value: 0.05<P<0.10)
2. Moderately significant (P value: 0.01
3. Strongly significant (P value: P≤0.01).
Results
The demographic features are presented in table 2. During this
study period, 16 patients were included [11 males and 5 females
(Figure 2) with mean age of 57.31 ± 9.88 years, the mean
duration of diabetes mellitus being 15.16 ± 7.61 years]. Left foot
was most commonly involved (43.8%). The prevalence of
~ 9 ~
~ 10 ~
National Journal of Clinical Orthopaedics www.orthoresearchjournal.com
hypertension was 75%, chronic kidney disease was 12.5% and
ischemic heart disease was 18.8%. 31.3% had acute Charcot
foot. 68.8% had single Joint involvement on radiographs (Figure
3) with pattern 3 of Charcot being commonest anatomic pattern
(Sander’s- Frykberg’s classification) affecting 75% of the cases
(Figure 4). Majority of the patients in this study had Amit Jain’s
type 1 Charcot foot (50%). 37.5% had some form of infection in
Charcot foot thereby complicating the Charcot foot and leading
to surgeries. 12.5% had underlying osteomyelitis and equal
percentage resulted in major amputation. 81.3% were on some
offloading (Table 2).
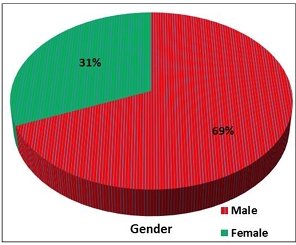
Fig 2: showing gender distribution
Table 2 showing demographic and characteristic profile
| Characteristics | NUMBER | PERCENTAGE |
|---|---|---|
| Age | 57.31 ± 9.88 | |
| Gender | ||
| Male | 11 | 68 |
| Female | 5 | 31.3 |
| Diabetes duration (Years) | ||
| < 10 | 2 | 12.5 |
| 10–20 | 13 | 81.3 |
| > 20 | 1 | 6.3 |
| Hypertension | ||
| Yes | 12 | 75 |
| No | 4 | 25 |
| Side of the foot | ||
| Right | 5 | 31.3 |
| Left | 7 | 43.8 |
| Bilateral | 4 | 25 |
| X-ray pattern of Charcot foot | ||
| Single | 11 | 68.8 |
| Mixed | 5 | 31.3 |
| Anatomical pattern of Charcot foot | ||
| Pattern I | 0 | 0 |
| Pattern II | 3 | 18.8 |
| Pattern III | 12 | 75 |
| Pattern IV | 1 | 6.3 |
| Pattern V | 0 | 0 |
| Amit Jain’s type of Charcot foot | ||
| Type 1 (Simple) | 8 | 50 |
| Type 2 (Complex) | 2 | 12.5 |
| Type 3 (Complicated) | 6 | 37.5 |
| Major amputation | ||
| Yes | 2 | 12.5 |
| No | 14 | 87.5 |
| Osteomyelitis | ||
| Present | 2 | 12.5 |
| Absent | 14 | 87.5 |
| Types of offloading | ||
| Total contact cast (TCC) | 2 | 12.5 |
| Removable Cast Walker (RCW) | 3 | 18.8 |
| Footwear | 4 | 25 |
| Amit Jain’s offloading | 4 | 25 |
| No offloading | 3 | 18.8 |
| Clinical type of Charcot | ||
| Acute | 5 | 31.3 |
| Chronic | 11 | 68.8 |
| Surgery done | ||
| Yes | 6 | 37.5 |
| No | 10 | 62.5 |
| Resurgeries done | ||
| Yes | 2 | 12.5 |
| No | 14 | 87.5 |
| Chronic kidney disease | ||
| Yes | 2 | 12.5 |
| No | 14 | 87.5 |
| Ischemic heart disease | ||
| Yes | 3 | 18.8 |
| No | 13 | 81.3 |
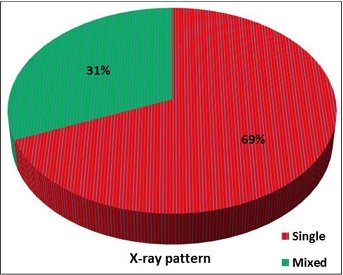
Fig 3: showing X-ray pattern distribution
No association was noted between age, gender, diabetes
duration, hypertension, side of foot, x-ray pattern, anatomical
pattern, osteomyelitis or major amputation with Amit Jain’s type
of Charcot foot (Table 3). Significant association was seen with
type of offloading used (P-0.003), clinical type of Charcot foot
(P-0.038) and surgery done (P<0.001) with Amit Jain’s type of
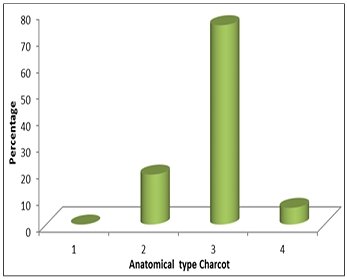
Fig 4: showing the anatomical pattern of Charcot foot
footwear was most commonly used offloading method in type 1
Charcot foot [Simple] whereas Amit Jain’s offloading system
was most commonly used offloading in type 3 Charcot foot (P
0.003). All the type 3 Charcot foot were chronic Charcot foot
and surgeries were done only in type 3 Charcot foot (Figure 5).
Table 3 : showing Association of clinical variables in relation to Amit Jain’s (AJ) Classification for Charcot foot
| Variables | Simple (n=8) | Complex (n=6) | Complicated (n=6) | Total (n=16) | P value |
|---|---|---|---|---|---|
| Age (years) | |||||
| 41–50 | 3 (37.5%) | 1 (50%) ) | 2 (33.3%) | 6 (37.5%) | 0.880 |
| 51–60 | 3 (37.5%) | 0 (0%) | 3 (50%) | 6 (37.5%) | |
| 61–70 | 1 (12.5%) | 0 (0%) | 0 (0%) | 1 (6.3%) | |
| 71–80 | 1 (12.5%) | 1 (50%) | 1 (16.7%) | 3 (18.8%) | |
| Gender | |||||
| Male | 5 (62.5%) | 1 (50%) | 5 (83.3%) | 11 (68.8%) | 0.615 |
| Female | 3 (37.5%) | 1 (50%) | 1 (16.7%) | 5 (31.3%) | |
| Diabetes Duration | |||||
| < 10 | 1 (12.5%) | 0 (0%) | 1 (16.7%) | 2 (12.5%) | 0.319 |
| 10-20 | 7 (87.5%) | 1 (50%) | 5 (83.3%) | 13 (81.3%) | |
| >20 | 0 (0%) | 1 (50%) | 0 (0%) | 1 (6.3%) | |
| Hypertension) | |||||
| Yes | 6 (75%) | 2 (100%) | 4 (66.7%) | 12 (75%) | 1.000 |
| No | 2 (25%) | 0 (0%) | 2 (33.3%) | 4 (25%) | |
| Side of the foot | |||||
| Right | 3 (37.5%) | 1 (50%) | 1 (16.7%) | 5 (31.3%) | 0.107 |
| Left | 5 (62.5%) | 43.8 | 0 (0%) | 2 (33.3%) | 7 (43.8%) |
| Bilateral | 0 (0%) | 1 (50%) | 3 (50%) | 4 (25%) | |
| X ray pattern of Charcot foot | |||||
| Single | 6 (75%) | 2 (100%) | 3 (50%) | 11 (68.8%) | |
| Mixed | 2 (25%) | 0 (0%) | 3 (50%) | 5 (31.3%) | |
| Anatomical pattern of Charcot foot | |||||
| Pattern I | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0.407 |
| Pattern II | 2 (25%) | 0 (0%) | 1 (16.7%) | 3 (18.8%) | |
| Pattern III | 6 (75%) | 1 (50%) | 5 (83.3%) | 12 (75%) | |
| Pattern IV | 0 (0%) | 1 (50%) | 0 (0%) | 1 (6.3%) | |
| Pattern V | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Major Amputation | |||||
| Yes | 0 (0%) | 0 (0%) | 2 (33.3%) | 2 (12.5%) | 0.233 |
| No | 8 (100%) | 2 (100%) | 4 (66.7%) | 14 (87.5%) | |
| Osteomyelitis | |||||
| Yes | 0 (0%) | 0 (0%) | 2 (33.3%) | 2 (12.5%) | 0.233 |
| No | 8 (100%) | 2 (100%) | 4 (66.7%) | 14 (87.5%) | |
| Types of Offloading | |||||
| TCC | 2 (25%) | 0 (0%) | 0 (0%) | 2 (12.5%) | 0.003** |
| RCW | 3 (37.5%) | 0 (0%) | 0 (0%) | 3 (18.8%) | |
| Footwears | 3 (37.5%) | 1 (50%) | 3 4 (25%) | ||
| Amit Jain’s Offloading | 0 (0%) | 1 (50%) | 3 (50%) | 4 (25%) | |
| No Offloading | 0 (0%) | 0 (0%) | 3 (50%) | 3 (18.8%) | |
| Clinical type of Charcot | |||||
| Acute | 5 (62.5%) | 0 (0%) | 0 (0%) | 5 (31.3%) | 0.038+ |
| Chronic | 3 (37.5%) | 2 (100%) | 6 (100%) | 11 (68.8%) | |
| Surgery Done | |||||
| Yes | 0 (0%) | 0 (0%) | 6 (100%) | 6 (37.5%) | <0.001** |
| No | 8 (100%) | 62.5 | 2 (100%) | 10 (62.5%) | |
| Resurgeries Done | |||||
| Yes | 0 (0%) | 0 (0%) | 2 (33.3%) | 2 (12.5%) | 0.233 |
| No | 8 (100%) | 2 (100%) | 4 (66.7%) | 14 (87.5%) | |
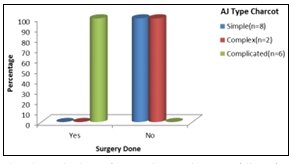
Fig 5: showing distribution of surgeries done according to type of Charcot foot
Major amputation occurred in type 3 Charcot foot and it had significant association (P-0.008) with osteomyelitis (Table 4).
| Variables | Yes (n=2) | No (n=14) | Total (n=16) | P value |
|---|---|---|---|---|
| Anatomical pattern of Charcot foot | ||||
| Pattern I | 0 (0%) | 0 (0%) | 0 (0%) | 1.000 |
| Pattern II | 0 (0%) | 3 (21.4%) | 3 (18.8%) | |
| Pattern III | 2 (100%) | 10 (71.4%) | 12 (75%) | |
| Pattern IV | 0 (0%) | 1 (7.1%) | 1 (6.3%) | |
| Pattern V | 0 (0%) | 0 (0%) | 0 (0%) | |
| Osteomyelitis | ||||
| Yes | 2 (100%) | 0 (0%) | 2 (12.5%) | 0.008** |
| No | 0 (0%) | 14 (100%) | 14 (87.5%) | |
| Chronic kidney disease | ||||
| Yes | 0 (0%) | 2 (14.3%) | 2 (12.5%) | 1.000 |
| No | 2 (100%) | 12 (85.7%) | 14 (87.5%) | 1.000 |
| Ischemic heart disease | ||||
| Yes | 0 (0%) | 3 (21.4%) | 3 (18.8%) | 1.000 |
| No | 2 (100%) | 11 (78.6%) | 13 (81.3%) | |
| Resurgeries | ||||
| Yes | 1 (50%) | 1 (7.1%) | 2 (12.5%) | 0.242 |
| No | 1 (50%) | 13 (92.9%) | 14 (87.5%) | |
| Clinical type of Charcot | ||||
| Acute | 0 (0%) | 5 (35.7%) | 5 (31.3%) | 1.000 |
| Chronic | 2 (100%) | 9 (64.3%) | 11 (68.8%) | |
| X-Ray pattern | ||||
| Single | 1 (50%) | 10 (71.4%) | 11 (68.8%) | 0.242 |
| Mixed | 1 (50%) | 4 (28.6%) | 5 (31.3%) | |
Table 4: showing association of variables of interest in relation to Major Amputation
Significant association was also seen between anatomical type
of Charcot foot and x ray pattern (P-0.018) wherein 90.9% of
pattern 3 Charcot had single joint involvement (Table 5).
Significant association was seen between type of offloading
used and clinical type of Charcot foot (P<0.001) and surgery (P
0.007). Removable cast walker and total contact cast was
significantly used in acute Charcot foot whereas therapeutic
footwear and Amit Jain’s offloading system was commonly used
in chronic Charcot foot. Amit Jain’s offloading was frequently
used in Charcot foot patients who underwent surgeries (Table 5).
One patient had history of failed Charcot reconstruction in the
past. There was no case of any peripheral arterial occlusive
disease and there was no mortality in this study.
| Variables of Interest | Osteomyelitis | Total (n=16) | P value | |
|---|---|---|---|---|
| Yes (n=2) | No (n=14) | |||
| X-Ray Pattern | ||||
| Single | 1 (50%) | 10 (71.4%) | 11 (68.8%) | 1.000 |
| Mixed | 1 (50%) | 4 (28.6%) | 5 (31.3%) | |
| Surgery Done | ||||
| Yes | 2 (100%) | 4 (28.6%) | 6 (37.5%) | 0.125 |
| No | 0 (0%) | 10 (71.4%) | 10 (62.5%) | |
| Anatomical type of Charcot foot (Sander’s–Frykberg’s) | ||||
| X-Ray pattern | ||||
| Single (n=11) | Mixed (n=5) | |||
| Pattern I | 0 (0%) | 0 (0%) | 0 (0%) | |
| Pattern II | 0 (0%) | 3 (60%) | 3 (18.8%) | 0.018* |
| Pattern III | 10 (90.9%) | 2 (40%) | 12 (75%) | |
| Pattern IV | 1 (9.1%) | 0 (0%) | 1 (6.3%) | |
| Pattern V | 0 (0%) | 0 (0%) | 0 (0%) | |
| Types of offloading used | ||||
| Total contact cast | 1 (9.1%) | 1 (20%) | 2 (12.5%) | 0.495 |
| Random cast walker | 2 (18.2%) | 1 (20%) | 3 (18.8%) | |
| Footwear | 4 (36.4%) | 0 (0%) | 4 (25%) | |
| Amit Jain’s offloading | 3 (27.3%) | 1 (20%) | 4 (25%) | |
| None | 1 (9.1%) | 2 (40%) | 3 (18.8%) | |
Table 5: showing association among different variables of interest
Discussion
Charcot foot in diabetes is a rare condition with lifetime
prevalence ranging from 0.1% to 10% [1]. It is invariably
associated with peripheral neuropathy in diabetes [6, 20].
Although, there is no gender predilection in Charcot foot, there
are studies where male gender was considered to be a risk factor
for Charcot foot [21]. It is seen often that Charcot foot develops in
diabetes usually after 10 years of duration [21]. The mean
duration of diabetes in our study was 15.56 years.
Although Charcot foot is seen frequently in one-foot, bilateral
presentation is also seen ranging from 9 to 75% in different
studies [21, 22]. In Salini et al. study [21], bilateral involvement
was seen in 18% whereas in our study around 25% had bilateral
Charcot foot. In Thewjitcharoen et al. series [23], acute Charcot
foot was seen in 33% and chronic Charcot was seen in 67%. In
our study, 31.3% had acute and 68.8% had chronic Charcot foot
(Figure 6).

Fig 6: Showing a chronic Charcot foot. This is Amit Jain’s type 1
Charcot foot (Simple)
According to Sander-Frykberg’s anatomical classification for
Charcot foot, there are 5 different patterns of which commonest
is pattern II (40%) followed by pattern III (30%) [6]. Even in
Thewjitcharoen et al series [23], pattern II was commonest seen
in 50% of cases followed by pattern III (27.5%). In our study,
75% of the cases had pattern III and only 18.8% had pattern II.
In Varma et al. study [21], 38% of the cases had single joint
involvement radiologic ally. In our study, 68.8% had single joint
involvement and 90.9% of the pattern III was significantly
associated with single pattern involvement.
It is seen that ulcerations and infection are common in Charcot
foot. As per Amit Jain’s classification for Charcot foot, presence
of ulcer renders a Charcot foot (Figure 7) as a complex Charcot
foot (type 2) and once infection sets in, the Charcot foot
becomes type 3 (complicated). Our study showed 37.5% of
Charcot foot is of complicated type. Around 5% to 51% of the
Charcot foot patients may require some form of surgery [22]. The
surgical options are debridement, exostectomy, arthrodesis and
amputation [22, 23]. There are evidence that <5% of the cases
require major surgical correction although in some series it can
be as high as 33% [23]. In Varma et al. series [22], around 9% of
the cases of Charcot foot required reconstructive foot surgeries.
In our series, none of the patients required any reconstructive
surgeries although one patient had past history of failed
reconstruction in acute Charcot foot. Studies have shown that
presence of ulcer in Charcot foot increased risk of major
amputation to more than 6 times compare to Charcot foot
without ulcer [23]. Around 37.5% of the patients underwent
surgeries in this series and all were done in type 3 Charcot foot
(significant association).
There were 2 major amputations (12.5%) and they were done in
type 3 Charcot foot (Complicated type). In Thewjitcharoen et al.
series [23], 13% of patients had osteomyelitis in Charcot foot.
Studies have shown that osteomyelitis is a major risk factor for
amputation [7]. In our study, 12.5% had osteomyelitis and it was
significantly associated with major amputation as osteomyelitis
is seen in type 3 Charcot foot.

Figure 7 Showing Amit Jain’s type 2 Charcot foot (Complex) Offloading remains mainstay of treatment in Charcot foot [1]. In
Thewjitcharoen et al. series [23], 85.7% of acute Charcot foot and
34.6% of chronic Charcot foot were on total contact cast. In our
series, total contact cast (40%) and removable cast walker (60%)
were used in acute Charcot foot and 36.4% of patients with
chronic Charcot foot had Amit Jain’s offloading system and foot
wear as offloading modality. Amit Jain’s offloading system was
significantly used as deflective offloading [13] in our patients
who underwent surgeries.
Conclusion
Charcot foot is a destructive disease which is uncommon and
frequently misdiagnosed. Majority of the cases in this study
were on simple type (Type 1). Total contact cast and Removable
cast walkers were most commonly used only in acute Charcot
foot whereas Amit Jain’s offloading system and Therapeutic
footwear were commonly used in chronic Charcot foot
especially in those patients who underwent surgery. All major
amputations were done in type 3 Charcot foot and osteomyelitis
was a significant contributing factor for major amputation as it
renders Charcot foot to a complicated type (Type 3). None of the
patients required reconstructive surgeries. Amit Jain’s extended
“SCC” classification for Charcot foot is a simple, practical, easy
to remember, focal classification of Charcot foot. It can serve as
an excellent teaching tool and also a good communicative tool.
It also helps in categorizing Charcot foot and provides a good
guide to treatment.
Acknowledgement
Authors would like to thank Dr. K.P. Suresh, Scientist
(Biostatistics), National Institute of Veterinary Epidemiology
and Disease Informatics (NIVEDI), Bangalore, India, for
reviewing the research methodology and statistical results of the
study and the Institutional ethics committee of RRMCH for
approving this study.
References
1.. Marmolejo VS, Arnold JF, Ponticello M, Andersen CA.
Charcot foot: Clinical clues, Diagnostic strategies and
Treatment principles. Am Fam Physician. 2018; 97(9):594
599.
2. Rosenbaum AJ, DiPreta JA. Classifications in Brief: Eichenholtz Classification of Charcot arthropathy. Clin Orthop Relat Res. 2015; 473:1168-1171.
3. Rogers LC, Frykberg RG, Armstrong DG, Boulton AJM, Edmonds M, Van GH et al. The Charcot foot in diabetes. Diabetes Care. 2011; 34:2123-2129.
4. Sohn MW, Lee Ta, Stuck RM, Frykberg RG, Mak EB. Mortality risk of Charcot arthropathy compared with that of diabetic foot ulcer and diabetes alone. Diabetes Care. 2009; 32(5):816-21.
5. Durgia H, Saboo J, Kamalanathan S, Palui R, Sridharan K, Raj H et al. Role of biphosphonates in the management of acute charcot foot. World J diabetes. 2018; 9(7):115-126.
6. Papanas N, Maltezos E. Etiology, Pathophysiology and classifications of the diabetic Charcot foot. Diabetic Foot & Ankle. 2013; 4:20872.
7. Viswanathan V, Kesavan R, Kavitha KV, Kumptla S. Evaluation of Roger’s Charcot foot classification system in South Indian Diabetic subjects with Charcot foot. J Diab Foot Comp. 2012; 4(3):67-70.
8. Jain AKC. Extended application of Amit Jain’s “SCC” classification concept for diabetic foot. Int J Surg Sci. 2019; 3(1):188-191. ~ 14 ~ National Journal of Clinical Orthopaedics www.orthoresearchjournal.com
9. Bevilacqua NJ. Current insights or classifying Charcot arthropathy. Podiatry Today. 2009; 22(40):22-29.
10. Jain AKC, Apoorva HC, Kumar H, Kumar K, Rajagopalan S. analyzing diabetic foot ulcer through amit Jain’s classification: A descriptive study. Int J Surg Sci. 2018; 2(4):26-32.
11. Jain AKC. A simple new classification for diabetic foot ulcers. Medicine Science. 2015; 4(2):2109-20.
12. Jain AKC. Amit Jain’s classifications for diabetic foot classifications. Saudi J Med. 2018; 3(1):1-5.
13. Jain AKC. Amit Jain’s classification for offloading the diabetic foot wounds. IJMSCI. 2017; 4(5):2922-5.
14. Jain AKC, Tejasvitaa RS. To determine the pattern and type of amputation done in diabetic foot patients in a teaching hospital. EAS J Med Surg. 2019; 1(3):94-99.
15. Gopal S, Haridarshan SJ. Amit Jain’s system of practice for diabetic foot: the modern diabetic foot surgery. Int J Res Orthop. 2019; 5(3):532-539.
16. Suresh KP, Chandrasekhar S. Sample Size estimation and Power analysis for Clinical research studies. J Human Rep Sc. 2012; 5(1):7-13.
17. Rosner B. In: Fundamentals of Biostatistics, 5th Edition, Duxbury, 2000.
18. Riffenburg RH. In: Statistics in Medicine, 2nd Edition, Academic press, 2005.
19. Rao PSSS, Richard J. In: An Introduction to Biostatistics, A manual for students in health sciences, New Delhi: Prentice hall of India. 4th Edition, 2006.
20. Petrova NL, Edmonds ME. Acute Charcot neuro osteoarthropathy. Diabetes Metab Res Rev. 2016; 32:281 286.
21. Salini D, Kumar H, Pillay M, Karimassery RS, Bal A, Chirukandath JS et al. Prevalence of charcot arthropathy in type 2 diabetes patients aged over 50 years with sever peripheral neuropathy: A retrospective study in a tertiary care South Indian Hospital. Indian J Endocr Metab. 2018; 107-11.
22. Varma AK, Jain AKC, Sandhya, Mangalanandan, Kumar H. Charcot foot in diabetes- a six month study from the largest limb salvage centre of the diabetes capital of the world. J Diab Foot Comp. 2016; 8(1):1-5.
23. Thwejitcharoen Y, Sripatpong J, Parksook W, Krittiyawong S, Porramatickul S, Srikummoon T et al. Salient features and outcomes of Charcot foot. An often-overlooked diabetic complications: a 17 year experience at a diabetic centre in Bangkok. J Clin Trans Endocr. 2018; 11:1-6.
2. Rosenbaum AJ, DiPreta JA. Classifications in Brief: Eichenholtz Classification of Charcot arthropathy. Clin Orthop Relat Res. 2015; 473:1168-1171.
3. Rogers LC, Frykberg RG, Armstrong DG, Boulton AJM, Edmonds M, Van GH et al. The Charcot foot in diabetes. Diabetes Care. 2011; 34:2123-2129.
4. Sohn MW, Lee Ta, Stuck RM, Frykberg RG, Mak EB. Mortality risk of Charcot arthropathy compared with that of diabetic foot ulcer and diabetes alone. Diabetes Care. 2009; 32(5):816-21.
5. Durgia H, Saboo J, Kamalanathan S, Palui R, Sridharan K, Raj H et al. Role of biphosphonates in the management of acute charcot foot. World J diabetes. 2018; 9(7):115-126.
6. Papanas N, Maltezos E. Etiology, Pathophysiology and classifications of the diabetic Charcot foot. Diabetic Foot & Ankle. 2013; 4:20872.
7. Viswanathan V, Kesavan R, Kavitha KV, Kumptla S. Evaluation of Roger’s Charcot foot classification system in South Indian Diabetic subjects with Charcot foot. J Diab Foot Comp. 2012; 4(3):67-70.
8. Jain AKC. Extended application of Amit Jain’s “SCC” classification concept for diabetic foot. Int J Surg Sci. 2019; 3(1):188-191. ~ 14 ~ National Journal of Clinical Orthopaedics www.orthoresearchjournal.com
9. Bevilacqua NJ. Current insights or classifying Charcot arthropathy. Podiatry Today. 2009; 22(40):22-29.
10. Jain AKC, Apoorva HC, Kumar H, Kumar K, Rajagopalan S. analyzing diabetic foot ulcer through amit Jain’s classification: A descriptive study. Int J Surg Sci. 2018; 2(4):26-32.
11. Jain AKC. A simple new classification for diabetic foot ulcers. Medicine Science. 2015; 4(2):2109-20.
12. Jain AKC. Amit Jain’s classifications for diabetic foot classifications. Saudi J Med. 2018; 3(1):1-5.
13. Jain AKC. Amit Jain’s classification for offloading the diabetic foot wounds. IJMSCI. 2017; 4(5):2922-5.
14. Jain AKC, Tejasvitaa RS. To determine the pattern and type of amputation done in diabetic foot patients in a teaching hospital. EAS J Med Surg. 2019; 1(3):94-99.
15. Gopal S, Haridarshan SJ. Amit Jain’s system of practice for diabetic foot: the modern diabetic foot surgery. Int J Res Orthop. 2019; 5(3):532-539.
16. Suresh KP, Chandrasekhar S. Sample Size estimation and Power analysis for Clinical research studies. J Human Rep Sc. 2012; 5(1):7-13.
17. Rosner B. In: Fundamentals of Biostatistics, 5th Edition, Duxbury, 2000.
18. Riffenburg RH. In: Statistics in Medicine, 2nd Edition, Academic press, 2005.
19. Rao PSSS, Richard J. In: An Introduction to Biostatistics, A manual for students in health sciences, New Delhi: Prentice hall of India. 4th Edition, 2006.
20. Petrova NL, Edmonds ME. Acute Charcot neuro osteoarthropathy. Diabetes Metab Res Rev. 2016; 32:281 286.
21. Salini D, Kumar H, Pillay M, Karimassery RS, Bal A, Chirukandath JS et al. Prevalence of charcot arthropathy in type 2 diabetes patients aged over 50 years with sever peripheral neuropathy: A retrospective study in a tertiary care South Indian Hospital. Indian J Endocr Metab. 2018; 107-11.
22. Varma AK, Jain AKC, Sandhya, Mangalanandan, Kumar H. Charcot foot in diabetes- a six month study from the largest limb salvage centre of the diabetes capital of the world. J Diab Foot Comp. 2016; 8(1):1-5.
23. Thwejitcharoen Y, Sripatpong J, Parksook W, Krittiyawong S, Porramatickul S, Srikummoon T et al. Salient features and outcomes of Charcot foot. An often-overlooked diabetic complications: a 17 year experience at a diabetic centre in Bangkok. J Clin Trans Endocr. 2018; 11:1-6.

