
INTRODUCTION
With increasing prevalence of diabetes
worldwide, its complication, the diabetic foot is also
increasing and it subjects a diabetic patient to a 10 to 30
times higher risk of extremity amputation (Jain, A. K. C.,
& Gopal, S. 2020; Kurup, R. et al., 2019). To prevent
complications and amputations, screening serves to be an
important strategy. However, it is well known in
literature that it is not practiced efficiently in most parts
of the world (Jain, A. K. C., & Gopal, S. 2020). Various
experts have proposed different screening tools for
diabetic foot from different parts of the world. Some of
the screening tool are Inlow’s 60 second screening tool,
simplified 60 second screening tool, Amit Jain’s 10 to 20
second screening tool/triple assessment, etc. All of them
have their own benefits and demerits but they aimed to
provide a method of screening (Jain, A. K. C. 2017; Jain,
A. K. C. et al., 2019).
The Inlow’s screening tool has a score ranging from 0 to 25 and patients have risk classification and recommendation of frequency of screening (Al- Lenjawi, B. et al., 2017).
The Amit Jain’s triple assessment, also known as Amit Jain’s 10 to 20 second screening tool, Amit Jain’s Linear foot test, Amit Jain’s screening tool, etc, was proposed in 2017 wherein minimum most parameters were suggested that were extremely essential in screening (Jain, A. K. C., & Gopal, S. 2020; Jain, A. K. C, 2017).
Different expert considers different parameters like rubor, erythema, fissures, blisters, etc to be essential in screening tool (Al-Lenjawi, B. et al., 2017; Woodbury, M. G., et al., 2015). Further, there are few who believe and suggest maceration, dermatitis, etc to be important and needs to be incorporated in screening tool (Al Lenjawi, B. et al., 2017). If one considers all of them, then one can imagine the burden a screening tool can face and they further can create literature confusions (Jain, A. K. C. 2014). In reality, many of the parameters are not essential when on consider screening tool protocols. Those parameters should consider in detail examination and not in screening.
The triple assessment for foot in diabetes has 3 simple parameters, the Look, the Feel and the Test component (LFT) that addresses the triopathy (Jain, A. K. C., & Gopal, S. 2020; Jain, A. K. C. et al., 2019). Studies done on this screening tool showed that even if parameters were downsized to just 3, only 6.7% to 7.7% of feet were evaluated in different studies done on this screening tool. The author proposes a new score for this screening tool which shall open new prospects for research on this scoring system for screening.
Figure 1 shows the new Amit Jain’s scoring for the LFT screening tool. The minimum score here is 0 and maximum score is 3 rendering it extremely simple to remember.
The Inlow’s screening tool has a score ranging from 0 to 25 and patients have risk classification and recommendation of frequency of screening (Al- Lenjawi, B. et al., 2017).
The Amit Jain’s triple assessment, also known as Amit Jain’s 10 to 20 second screening tool, Amit Jain’s Linear foot test, Amit Jain’s screening tool, etc, was proposed in 2017 wherein minimum most parameters were suggested that were extremely essential in screening (Jain, A. K. C., & Gopal, S. 2020; Jain, A. K. C, 2017).
Different expert considers different parameters like rubor, erythema, fissures, blisters, etc to be essential in screening tool (Al-Lenjawi, B. et al., 2017; Woodbury, M. G., et al., 2015). Further, there are few who believe and suggest maceration, dermatitis, etc to be important and needs to be incorporated in screening tool (Al Lenjawi, B. et al., 2017). If one considers all of them, then one can imagine the burden a screening tool can face and they further can create literature confusions (Jain, A. K. C. 2014). In reality, many of the parameters are not essential when on consider screening tool protocols. Those parameters should consider in detail examination and not in screening.
The triple assessment for foot in diabetes has 3 simple parameters, the Look, the Feel and the Test component (LFT) that addresses the triopathy (Jain, A. K. C., & Gopal, S. 2020; Jain, A. K. C. et al., 2019). Studies done on this screening tool showed that even if parameters were downsized to just 3, only 6.7% to 7.7% of feet were evaluated in different studies done on this screening tool. The author proposes a new score for this screening tool which shall open new prospects for research on this scoring system for screening.
Figure 1 shows the new Amit Jain’s scoring for the LFT screening tool. The minimum score here is 0 and maximum score is 3 rendering it extremely simple to remember.
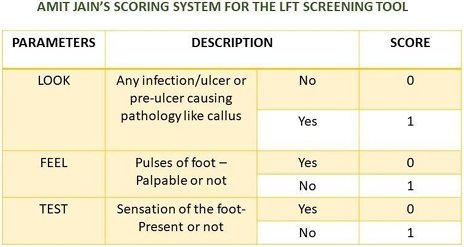
Figure 1 showing the new simple scoring for the Amit Jain’s triple assessment for foot in diabetes
A quarterly, semi-annually and annual follow
up can be done by respective health care professional
based on risk group and the single assessment and double
assessment should be considered during follow- up. Just
the way the author had given a coding system for diabetic
foot ulcer similar to TNM staging concept
(Jain, A, K, C. 2020), one can consider a coding system
for this LFT screening tool (Figure 2). One can easily use
the coding in their practice as there are just 3 parameters
rendering it efficient in remembering and documenting
this screening tool

Figure 2: showing the plantar view of left foot (Look Component). Left great toe has callus, there is severe underlying
neuropathy and pulses are palpable. As per Amit Jain’s coding it is L1F0T1 (or L1F0T1). The Amit Jain’s score is 2.
CONCLUSION
Amit Jain’s triple assessment is one of the
simplest screening tools that addresses the triopathy in
diabetic foot and it has minimum parameters that are
essential. Adding a score to the LFT screening is done to
open further prospects for research on this screening tool.
REFERENCES
1. Jain, A. K. C., & Gopal, S. (2020). Comparing foot
evaluation in hospitalized diabetic patients between
surgeons, orthopedicians and physicians through
Amit Jain’s triple assessment. East African Scholars
J Med Sci, 3(5), 169-178.
2. Kurup, R., Ansari, A. A., Singh, J., & Raja, A. V. (2019). Wound care knowledge, attitudes and practice among people with and without diabetes presenting with foot ulcers in Guyana. The Diabetic Foot Journal, 22(3), 24-31.
3. Jain, A. K. C. (2017). Amit Jain’s triple assessment for foot in Diabetes – the simplest and the fastest new screening tool in the world. IJMSCI, 4(6), 3015 19.
4. Jain, A. K. C., Apoorva, H. C., & Kumar, K. (2019). Screening of diabetic foot through Amit Jain’s triple assessment: A 10 to 20 second screening method. Int J Orthod Sci, 5(2), 227-229.
5. Al-Lenjawi, B., Mohamed, H., & Azmy, A. (2017). Is it time to reconsider the 60 seconds diabetic foot screen reorganizing the 60 second foot exam for people with diabetes? Dermatol Open J, 2(1), 10- 15.
6. Woodbury, M. G., Sibbald, R. G., & Ostrow, B. (2015). Tool for rapid easy identification of high- risk diabetic foot: Validation and clinical pilot of the simplified 60 second diabetic foot screening tool. Plos One, 10(6), e0125578.
7. Jain, A. K. C. (2014). A new staging system for cellulitis in diabetic lower limbs – improving diabetic foot practice around the world. J Diab Foot Comp, 6(2), 48-53.
8. Jain, A. K. C. (2020). Development of a new Amit Jain’s scoring system for diabetic foot ulcer. IAR J Med Sci, 1(1), 31-34.
2. Kurup, R., Ansari, A. A., Singh, J., & Raja, A. V. (2019). Wound care knowledge, attitudes and practice among people with and without diabetes presenting with foot ulcers in Guyana. The Diabetic Foot Journal, 22(3), 24-31.
3. Jain, A. K. C. (2017). Amit Jain’s triple assessment for foot in Diabetes – the simplest and the fastest new screening tool in the world. IJMSCI, 4(6), 3015 19.
4. Jain, A. K. C., Apoorva, H. C., & Kumar, K. (2019). Screening of diabetic foot through Amit Jain’s triple assessment: A 10 to 20 second screening method. Int J Orthod Sci, 5(2), 227-229.
5. Al-Lenjawi, B., Mohamed, H., & Azmy, A. (2017). Is it time to reconsider the 60 seconds diabetic foot screen reorganizing the 60 second foot exam for people with diabetes? Dermatol Open J, 2(1), 10- 15.
6. Woodbury, M. G., Sibbald, R. G., & Ostrow, B. (2015). Tool for rapid easy identification of high- risk diabetic foot: Validation and clinical pilot of the simplified 60 second diabetic foot screening tool. Plos One, 10(6), e0125578.
7. Jain, A. K. C. (2014). A new staging system for cellulitis in diabetic lower limbs – improving diabetic foot practice around the world. J Diab Foot Comp, 6(2), 48-53.
8. Jain, A. K. C. (2020). Development of a new Amit Jain’s scoring system for diabetic foot ulcer. IAR J Med Sci, 1(1), 31-34.

