Address for Correspondence: Dr Ajit Kumar Varma, Professor, Department
of Endocrinology, Diabetic lower limb and Podiatric surgery
Amrita Institute of Medical Sciences,
Amrita Vishwa Vidyapeetham University
Ponekara P.O, Kochi-682041, Kerala, India.
Email- ajitkumarvarma@aims.amrita.edu
1 MBBS,DNB[Gen Surgery],(Postdoctoral Fellow in Diabetic Lower Limb
and Podiatric Surgery]
2 MBBS,MS[Gen Surgery],(Professor)
3 DPA,(Podiatry Assistant)
4 MBBS,(Associate Professor)
5 MBBS,DNB,MRCP[Professor and HOD)
Department of Endocrinology, Diabetic Lower Limb and Podiatric Surgery,
Amrita Institute of Medical Sciences, Amrita Vishwa Vidyapeetham,
Ponekara P.O, Kochi, Kerala, India.682041
INTRODUCTION
INTERNATIONAL DIABETIC FOOT PRO JECTS
INTRODUCTION
Necrotizing fasciitis is a rare soft tissue infection involving primarily the superficial fascia and resulting in extensive undermining of soft tissue. It is perhaps the most aggressive form of soft tissue infection1 and can spread rapidly to involve the whole limb within hours.2 This disease has bewildered physicians for centuries. Hippocrates in the fifth century B.C gave the first description of this dreaded infection.3
The term necrotizing fasciitis was first introduced by Wilson4 in 1952 and is the preferred term today describing the most consistent and key feature of this disease, fascial necrosis. In the 1990’s, necrotizing fasciitis became popularly known in media as the “flesh eating bacteria disease”.5
The mortality rates of this disease have remained alarmingly high with reported mortality rates ranging from 6 to 76%.6 It is the delay in the diagnosis and consequently delayed operative debridement that has been shown in multiple studies to increase the mortality.7-13 One of the main reasons for the continued high mortality of patients affected by this disease is failure to recognize and diagnose the condition early.
Although considered rare, it is frequent enough that surgeons will have been involved with the management of at least one patient with necrotizing fasciitis during their practice.14
The Journal of Diabetic Foot Complications
Necrotizing fasciitis occurs commonly in diabetes mellitus, alcoholics, AIDS, malignancy and intravenous drug abusers. It commonly involves the abdomen, perineum, scrotum and extremities.
This study investigates the surgical outcome of necrotizing fasciitis exclusively in the diabetic lower limb over a one year time period in our center. To our knowledge this is probably one of the largest series of necrotizing fasciitis reported, especially in diabetic lower limbs.
Patients and Methods
This retrospective study included all the ents admitted and treated in our rd for necrotizing fasciitis from January 2008 through December 2008.
Amrita Institute of Medical Sciences and Research Centre at Kochi, India is a large tertiary, superspecialty referral hospital with 1450 Inpatient beds. Our department is the only one of its kind in India with a well established Podiatric Surgery wing. The division of Podiatric Surgery is partnered with the department of Endocrinology and Diabetes. This integrated team approach, so important in the proper management of diabetic lower limb problems, is available in only a few centres worldwide. Our daily In-patient census is around 40 to 45 patients and our daily Outpatient turnover is around 50-60 patients. We encounter necrotizing fasciitis very frequently, about one case every week.
Our ability to diagnose necrotizing fasciitis clinically has improved with years of experience in managing this disease. The diagnosis was made by a combination of clinical and gross anatomical findings during surgery. Only in difficult cases where the clinical diagnosis is not obvious do we resort to MRI or CT scan for confirmation. The following were the inclusion and exclusion criteria for our study:
Inclusion criteria
1. Type 2 diabetes.
2. Necrotizing fasciitis affecting the lower limb in
patients who underwent surgery at our institution.
Exclusion criteria
1. Necrotizing fasciitis in non diabetic persons.
2. Necrotizing fasciitis in diabetic persons involving other sites.
3. Conservatively managed early necrotizing fasciitis
4. Cases of necrotizing fasciitis with insufficient data for our study.
Results
R A total of 609 patients had undergone surgery for diabetic lower limb infections during the study period. Of 53 patients with necrotizing fasciitis in the index year, 44 patients met the criteria to be included in the study. Thus the incidence of necrotizing fasciitis in patients undergoing surgery for infection in our center is approximately 7.25%.
Our patients were predominantly men (76.09%), with the male to female ratio being 3:1. The mean age of males and females undergoing surgery for necrotizing fasciitis was 58.12 years (range 32-88 years) and 57.28 years (43-72 years), respectively. (TABLE 1)
The total number of surgeries done on the 44 patients with necrotizing fasciitis was 53. The surgeries included debridement, below knee and above knee amputations. The most common procedure done was debridement (66.03%). Above knee amputation was required in 16.98% and 7.5%of patients underwent below knee amputation. One patient underwent a revision to a below knee amputation (1.9%). Thus, the incidence of major amputation was 26.4%. (TABLE 2)
| SEX | NUMBER | PERCENTAGE |
|---|---|---|
| Male | 33 | 76.09% |
| Female | 11 | 23.91% |
| Total | 41 | 100% |
Table 1 The distribution of lower limb necrotizing fasciitis in diabetic males and females.
| SURGERY | NUMBER | PERCENTAGE |
|---|---|---|
| Total debridement | 35 | 66.03% |
| Toe amputation | 03 | 5.6% |
| Toe amputation | 01 | 1.9% |
| Foot amputation | 04 | 7.5% |
| Below knee amputation | 09 | 16.98% |
| Revision surgery[Amputation] | 01 | 1.9% |
| Total | 44 | 100% |
| PATIENTS | NUMBER | PERCENTAGE |
|---|---|---|
| Dead | 3 | 6.81% |
| Alive | 41 | 93.19% |
| Total | 44 | 100% |
Discussion
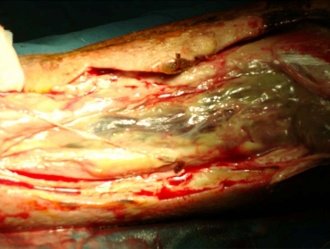
Figure 1 Intra-operative photos of a case of necrotizing fasciitis undergoing radical debridement. Note the extensive necrosis of the fascia with fluid collection.
A high index of suspicion is required to diagnose necrotizing fasciitis. Tenderness, redness and raised local temperature are the common signs in the early stage. As the infection extends, the overlying skin becomes smooth, shiny and tensely swollen. Within one or two days, the lesions’ color changes from red to purple to blue and become frankly gangrenous by the 4th-5-th day. In clostridial infections, crepitance suggests the production of gas. The infection progresses to nerve necrosis with hypoaesthetic or anaesthetic skin areas.15 The patient then progresses to sepsis and septic shock. Radical debridement (FIGURE 1) is the cornerstone to the management of this disease.
All patients who present to our Institute with necrotizing fasciitis are immediately started on empirical broad-spectrum antibiotics after adequate resuscitation. The initial empirical antibiotic protocol at our department for necrotizing fasciitis consists of a combination of Piperacillin Tazobactam, Clindamycin and Linezolid. This antibiotic protocol is, however, renewed every year as per the changing bacteriological flora. In the absence of sepsis or an acute emergency, the infection is allowed to localize and within 24 to 48 hours patient is taken up for surgery.
The incidence of NF in the United States has been reported to be 0.53 cases per 100,0002 , while the incidence at our institute was around 7.25% just in lower limbs of diabetic patients. The frequency of necrotizing fasciitis is increasing in India. Around 70% of the population in India lives in rural areas. Barefoot walking, inappropriate foot wear usage, lack of awareness of the seriousness of diabetic foot problems, rat and insect bites, and vigorous massage all predispose the patients to necrotizing fasciitis.16,17
Tang et.al2 in their series of 24 patients with necrotizing fasciitis of the limbs in which 12 cases involved lower limb, reported a mortality of 53.3%. Wong et.al7 in their series of 89 patients, 70% of which involved the lower limbs, had a mortality rate of 21.3%. When compared to these and other studies reporting mortality rates of 6-76%, the mortality due to necrotizing fasciitis at our institute was only 6.8%. We attribute this lower mortality to our combined multidisciplinary approach towards management of diabetic foot infections wherein the multidisciplinary team chiefly consists of podiatric surgeons, diabetologists, intensivists and other specialties as needed and when required.
References
1. Chin Ho Wang, Yi Shi Wang. The diagnosis of necrotizing fasciitis. Curr Opin Infect Dis 2005;18:101-106.
2. Tang W.M, Ho P.L, Fung K.K, Yuen K.Y, Leong J.C.Y. Necrotizing fasciitis of a limb. J Bone Joint Surg 2001;83-B:709-14.
3. Descamps V, Aitken J, Lee MG, Hippocrates on necrotizing fasciitis. Lancet 1994; 344:556.
4. Wilson B. Necrotizing fasciitis. Am Surg 1952;18:416.
5. Childers BJ, Potyondy LD, Nachreiner R, Rogers FR, Childers ER, Oberg Kg, et.al. Necrotizing fasciitis: a fourteen year retrospective study of 163 consecutive patients. Am Surg 2002;68(2):109-16.
6. McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA. Determinant of mortality in necrotizing soft tissue infections. Ann Surg 1995;221:558-563.
7. Wong CH, Chang HC, Pasupathy S, et.al. Necrotizing fasciitis: clinical presentation, microbiology and determinants of mortality. J Bone Joint Surg , Am 2003;85A:1454-1460.
8. Voros D, Pissiotis C, Georgantas D, et.al. Role of early and aggressive surgery in the treatment of severe necrotizing soft tissue infections. Br J Surg 1993;80:1190-1191.
9. Rea WJ, Wyrick WJ. Necrotizing fasciitis. Ann Surg 1970;172:957-964.
10. Green RJ, Dafoe DC, Rafffen TA. Necrotizing fasciitis. Chest 1996;110:219-229.
11. Wang K-C, Shih C.H. Necrotizing fasciitis of the extremities. J Trauma 1992;32:259-264.
12. Majeski J, Majeski E. necrotizing fasciitis: improved survival with early recognition by tissue biopoy and aggressive surgical treatment. South Med J 1997;90:1065-1068.
13. Elliot DC, Kufera JA, Myers RA. Necrotizing soft tissue infections : risk factors for mortality and strategies for management . Ann Surg 1996;224:672-683.
14. Nagvi GA, Malik SA, Jan W. Necrotizing fasciitis of the lower extremity : a case report and current concept of diagnosis and management. Scand J Trauma Resuce Emerg med 2009;17:28.
15. Smeets L, Bow A, Heyman O. Necrotizing fasciitis: case report and review of Literature. Acta Chir BElg 2007;107:29-36.
16. Vijay V, Snehalatha C, Ramamchandran A. Socio-cultural practices that may effect the development of the diabetic foot. IDF Bulletin 1997:42:10-2.
17. Vijay V, Narasimham A, Senna R, Snehalatha C, Ramachandran A. Clinical profile of diabetic foot infections in South India- A retrospective study. Diabetic Medicine 2000;17:215

